|
a faculty
teaches how to learn
and Life is
an eternal faculty,
from which
you must never graduate
and will
eternally earn...
- dr. yalcin ergir (Life)
RIGHT HERE WAITING FOR YOU…
LIVE and ALIVE orthodontic
eruption story of an impacted canine
(periodical case
report)
Lecture for Dental Students –
by
Dr. Yalcin Ergir - Orthodontist - Turkey

an
impacted canine in maxilla,
only
gives up resistance and erupts -
if it
is a: “canine in love”
**
** **
FESTINA LENTE
If you are planning to erupt an
impacted canine by means of orthodontic treatment;
besides having to be very kind to the
tissues surgically -
you must “slowly” apply gentle
orthodontic forces to the impacted canine &
you must “hurry” to take the short
way home, with frequent clinical controls.
Not only canine; but every single
tooth is valuable and of course:
“own” healthy tooth, with a healthy
periodontium is always eternally much more precious than:
“stranger” endosseous implant
supported restorations.
After puberty, if a maxillary canine
tooth shows no sign of eruption, the area must be
examined clinically and radiologically.
The position of the canine (the
angular degree: whether it is horizontal, oblique or
vertical),
the necessary space at the dental
arch,
the bone structure & the health of
the periodontal tissues,
will guide us in making in a plan in:
a- extraction or non-extraction of a
first premolar tooth (/or a persistent deciduous canine
/or both)
b- the surgical coordinates of soft
tissues & bone
c- the orthodontic appliance systems
and force vectors
d- the average period of the
orthodontic journey and full treatment
ORTHODONTIC ERUPTION
The best treatment is prevention. The
prevention begins with eliminating the potential factors
if possible, before the natural eruption time.
This may be early extraction of a
deciduous canine or maybe root cannot be resorbed by the
permanent canine developing in an unnatural position and
direction.
If this timing is missed and if the
canine has not erupted long after puberty; it has to be
tracked slowly to its original place in the dental arch
like a White Submarine, which has to go “20000
Leagues Under the Sea”.
This treatment or this long journey
may take between a year or two –
there may be multiple surgical
operations at the beginning if the bonded bracket breaks
deep inside the cavity.
Long term patient cooperation is
essential as long term use of braces hygienically needs
great discipline and social self-confidence as well.
BUT IT IS WORTH IT; when it safely and
gloriously reaches to his corner at the harbor of the
mouth.
It is your own tooth, it is vital; it
can feel cold of ice-cream, the heat of coffee, the
hardness of an apple with its micro neurovascular system.
If it is obvious that the impacted
canine will not be able to make a healthy inter-bone
journey or will harm other teeth- still another
transportation and eruption method must be considered in
treatment planning, before extraction and titanium
implant applications: AUTOTRANSPLANTATION.
AUTOTRANSPLANTATION
Auto-transplantation of impacted (or
embedded) canine tooth is the fastest way to carry the
tooth to its original position on the dental arch – in
proper dental alignment.
In autotransplantation, after the
impacted canine tooth is reached by surgical means, it
is kindly extracted in one piece – the root is filled by
endodontic treatment and the extracted canine is
implanted to the surgically prepared artificial cavity (or
extracted deciduous tooth cavity) immediately.
Devital canine must be fixed to the
neighbor teeth, till it reaches stability in its new
alveoli. This fixation has to remain lifelong in “misforecasted”,
“misplanned”, or “mistreated” applications.
This method is fast; BUT the tooth is
no more vital afterwards. Beside the loss of
proprioception, there are always risks of: fusion,
fragility, cystic or inflectional pathologies in the
future.
TITANIUM IMPLANTATION
Similar potential problems of a
titanium implant supported restoration may bring
esthetical dissatisfactions along as well.
“Healthy” & “Own” are 2 important
keywords in our choice;
when an impacted canine in love with
you is waiting to be erupted
and while you’re right there waiting
for it.
DOING NOTHING AT ALL
Perhaps to decide whether “to begin”
or “not to begin” a treatment is more important than
deciding a method for treatment.
Every impaction is like a fingerprint:
UNIQUE - in its circumstances.
So in some cases “doing nothing at
all”, may be the best treatment method,
when local and systemic disease
conditions are thoroughly observed.
If the canine is left impacted; there
will always be a slight risk of leaving a pathogenic
source for the future; but if it seems obvious that:
“Doing an orthodontic treatment”
will give more harm than:
“Not doing an orthodontic treatment”
–
“Doing nothing at all” will be
the most healthy or least harmful choice, like:
“Making love out of nothing at all”.
WANTED; DEAD OR ALIVE?
“Healthy” suits “Alive”, much more
than it suits “Dead”.
Listening to a song “Live” (even with
mistakes) in a concert is much warmer than:
listening to a studio recorded,
million times corrected industrial song.
For a dental student; learning a
treatment method:
step by step “Live” & being explained
“as” the treatment continues –
may be much more educational than
reading an already completed case report.
SO
HERE IS OUR FAITHFUL TOOTH FAIRY

SO
HERE ARE STEP BY STEP EXPLAINED LIVE STAGES OF A SLOW
-
BUT VITAL (ALIVE) TREATMENT CHOICE,
IN
ERUPTING AN IMPACTED MAXILLARY CANINE TOOTH
OF
A 21 YEAR OLD ADOLESCENT:
2011-07-22
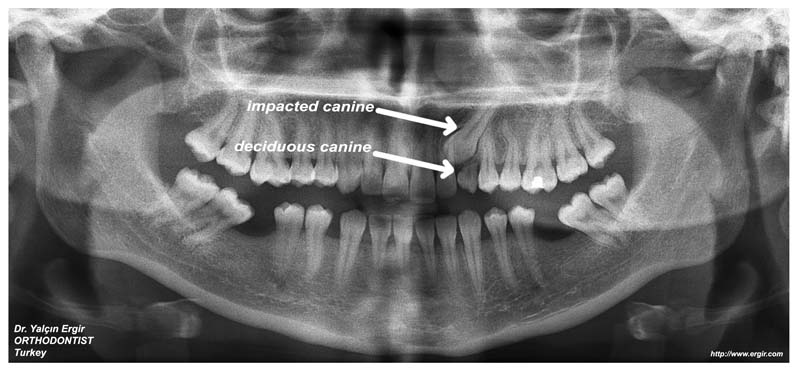
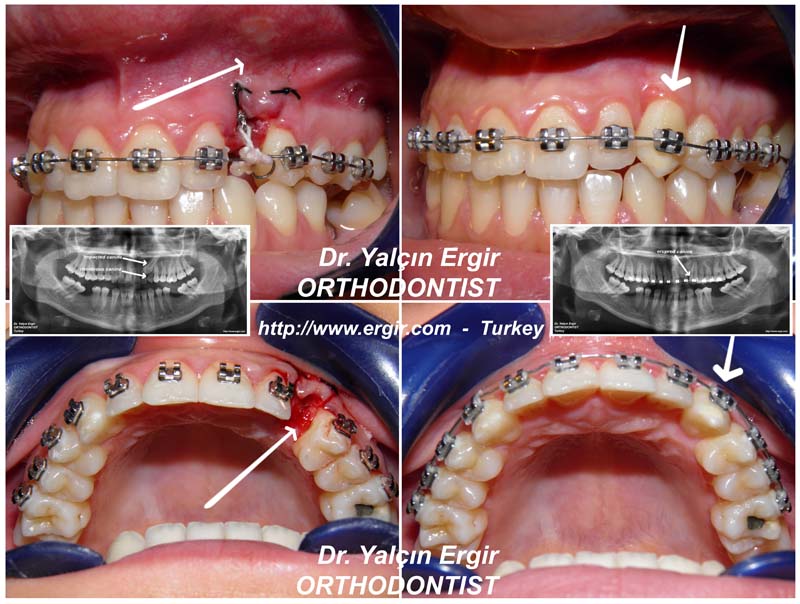
At the clinical examination of the
patient’s dental structure, an upper left persistent
deciduous canine tooth is seen.
The anamnesis has no information
about an erupted or extracted permanent canine tooth.
Panoramic radiograph shows the
impacted permanent canine tooth in semi-oblique position,
and the deciduous canine’s half resorbed short &
untrustworthy
root. There is luxation at the deciduous canine in
manual inspection as well.
There is no systemic disease and the
periodontal status is perfect. The young bone structure
of 21 year old patient will help us in choosing the
Vital - ORTHODONTIC ERUPTION treatment method.
We can begin our long journey;
hope the impacted canine will feel
the good wishes
and will give up its resistance, its
eternal impaction with love.
After the location of the canine deep
inside is determined,
in order to do the maximum bonding
job before bleeding occurs by surgical reaching to
impacted canine the maxillary teeth are cleaned and the
brackets are bonded to the teeth (except deciduous
canine, because it has to be extracted at the beginning
of the surgical operation)

The necessary vestibule gingival
region (the palate in most impacted canine cases) is
anesthetized. The deciduous tooth is extracted. With
surgical incision, the vestibule flap is lifted and a
window is opened at the bone to reach the enamel of the
impacted canine tooth.
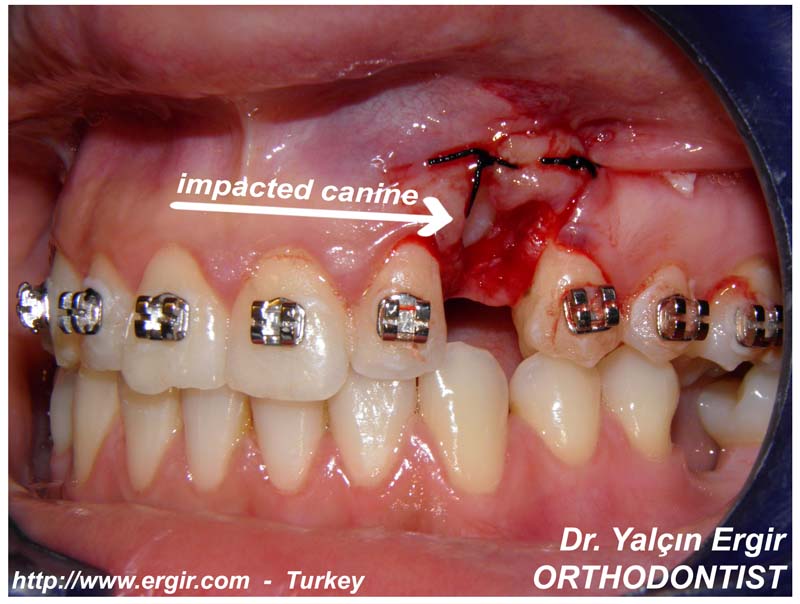
After the suturing, the impacted
canine is ready to be bonded and ready for orthodontic
forces.
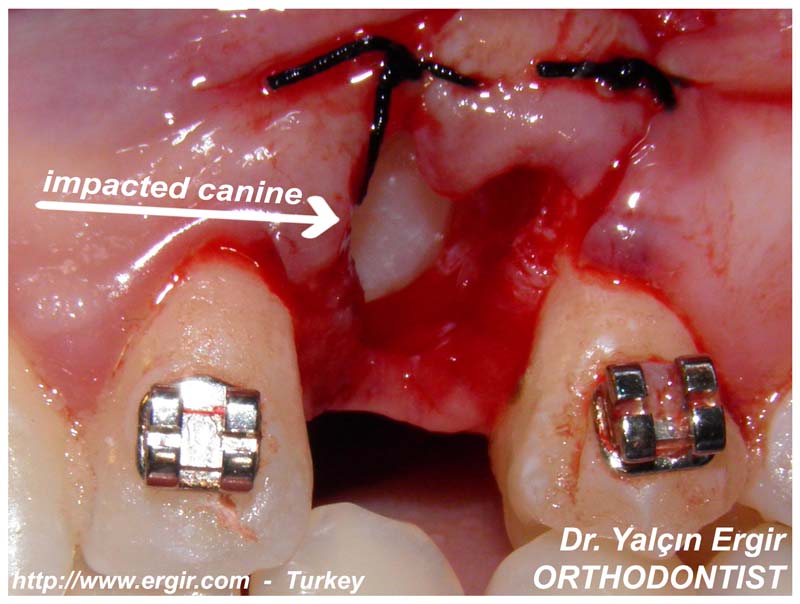 
(surgery:
Dr. Merih Baykara)
The surgically obtained soft tissue
window tends to close within days while healing; so the
bracket must be bonded as soon as the tooth can be
reached.
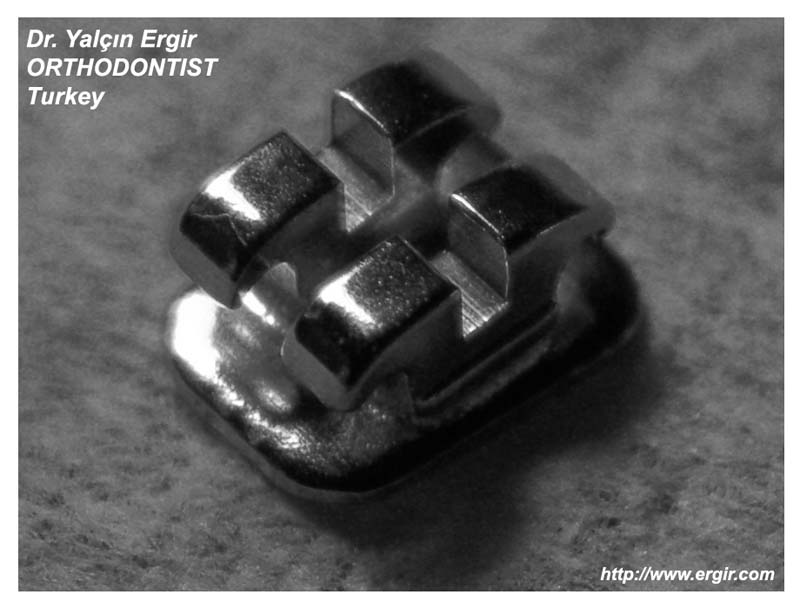
The necessary area for an
orthodontist on the canine is not squares of meters:
just to expose 4X3 millimeters of
enamel area for bonding a tiny bracket is enough.
After the control of bleeding and the
moment the surface can be kept dry – the bracket,
preferably metal mandibular incisal bracket (not ceramic,
for maximal endurance and minimal dimension factors) is
bonded to the enamel of the canine.
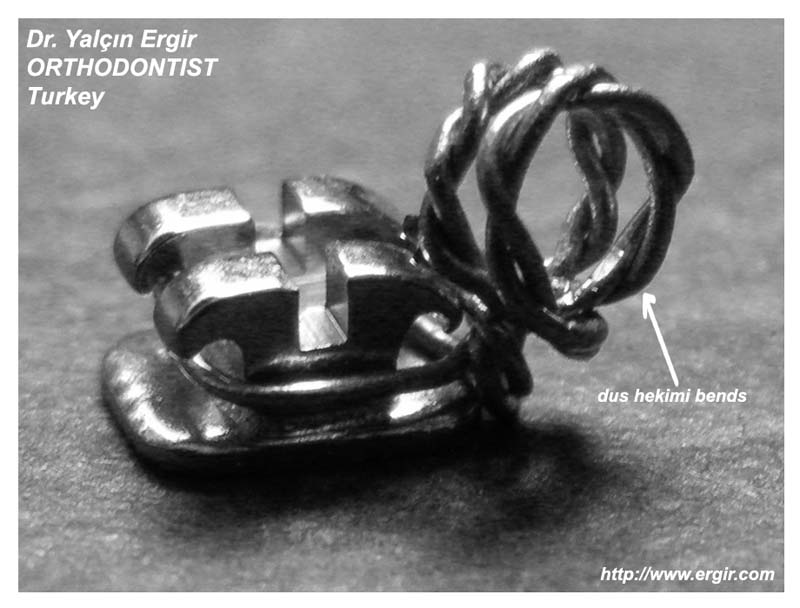
The bracket must be specially
prepared before surgery
and suitable (+ reachable) anchorage
points must be constituted.
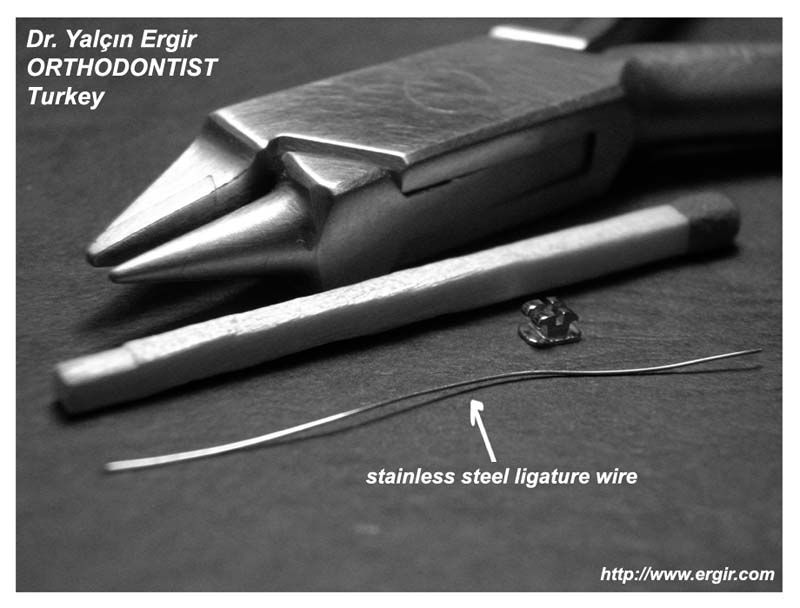
Within years of experience, I think
the best system is forming a “double loop” by a (Ø 0,25") stainless steel ligature wire and tie it to the
bracket before bonding.
A double loop with twisted wire will
suspend the unwanted forces during eating and will
decrease the breaking risk. This suspension will
additionally act as an active wire and will be giving a
continuous gentle pulling force to the impacted canine
tooth.
During the bonding process, you must
pay great attention to bleeding and moistening, as it
will be very hard to re-bond the broken bracket at the
beginning of the treatment, while the impacted canine is
still lying deep inside - covered with fragile tissues.
The titanium wire cannot be applied
to the maxillary teeth’s brackets if the surgical
interference should be applied from the vestibule region;
so the wire must be put after the surgery and bonding is
completed.
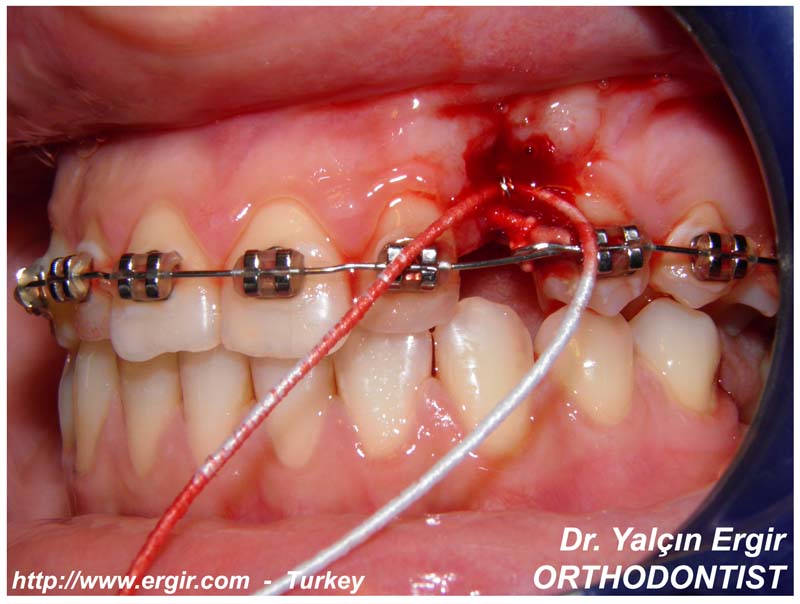
A loop to an appropriate region can
be formed on the titanium wire, so that it can pull the
impacted tooth’s bracket in a proper vector by elastic
threads or coil springs.
In this case, twin elastic threads
are applied between the loops of the impacted canine and
the (Ø 0,16") NI-TI wire.
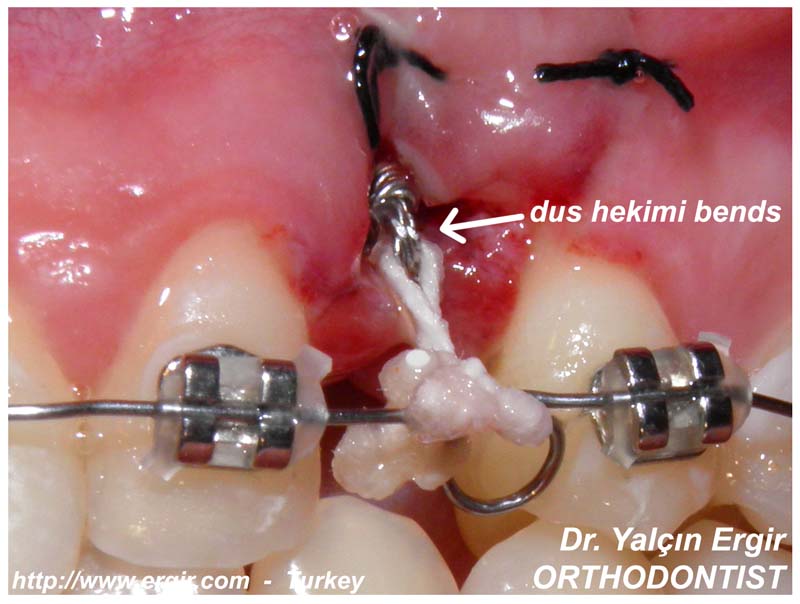 
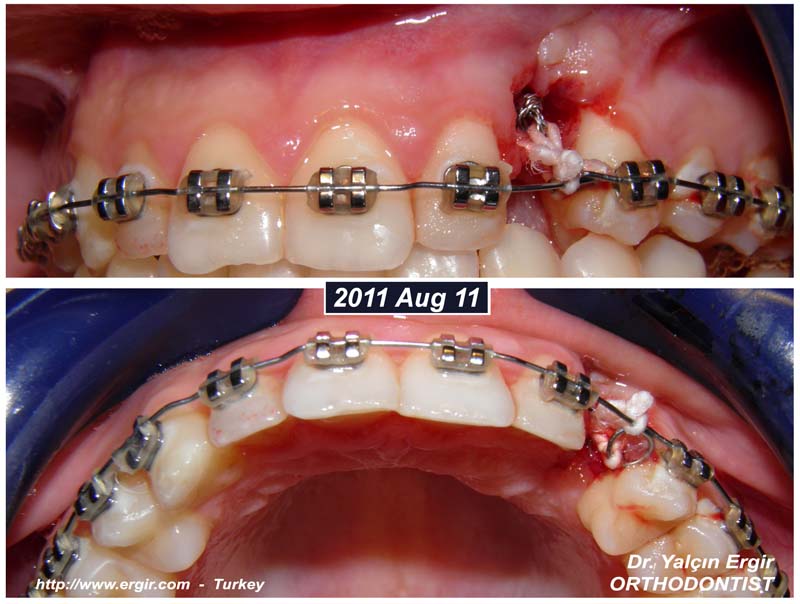
2011-08-11
2 weeks later, the hypertrophic scar
is excised and the new twin elastic threads are applied
from the exposed bracket loops - to the titanium wire
and its loop. We must apply even more gentle forces in
these semi-blind & damp circumstances, in order not to
re-bond a bracket if it breaks.
(surgery:
Dr. Yalcin Ergir)
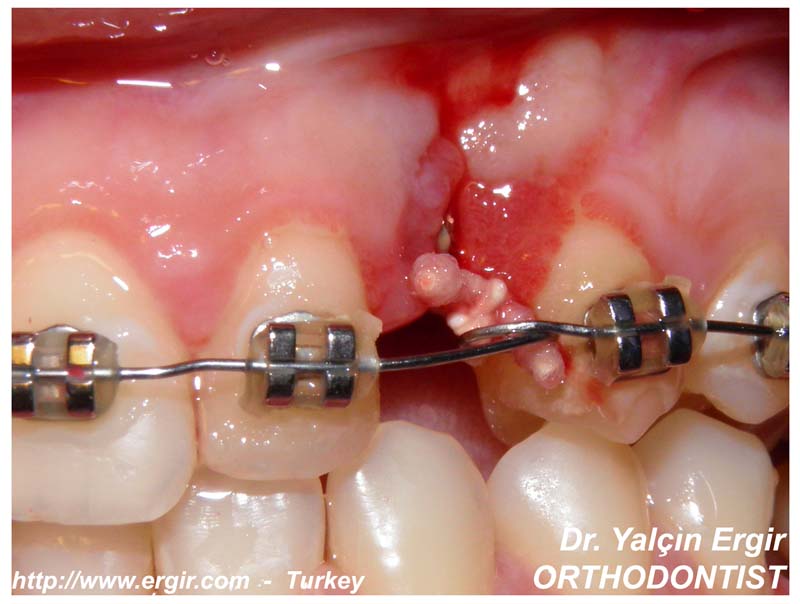
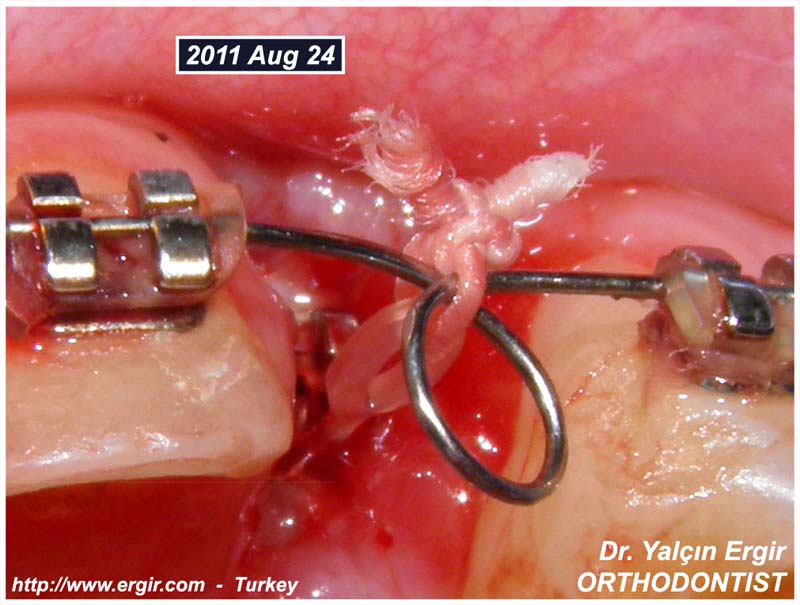
2011-08-24
it's
coming; it's coming!...
A little
smile can let all the sunshine in.
Now we
must festina lente – hurry, slowly.
Canine is
no more "that deep"; there is no more need for a loop with Dus
Hekimi Bends. We can easily reach and apply our force
directly to the bracket.
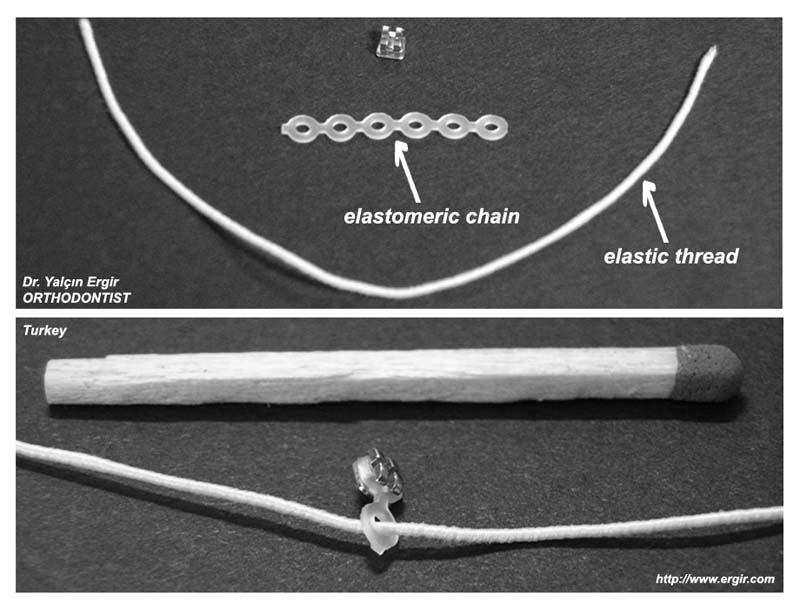
If we tie
an “elastic thread” to the bracket, it cannot wrap the
bracket properly at the bottom side - which needs a
vertical and labial pulling force vector.
So we can
use an “elastomeric chain” which will perfectly wrap the
bracket and afterwards we can apply elastic thread’s
pulling force to the elastic chain.
For that,
we have to insert the thread to the chain, like
inserting into a sewing needle.
Now we can
sing: “I’ve Got The Power!...”
All we have to do is to stretch the
thread (& chain) towards the Ni Ti wire.

And put a sailor’s knot for our
submarine.
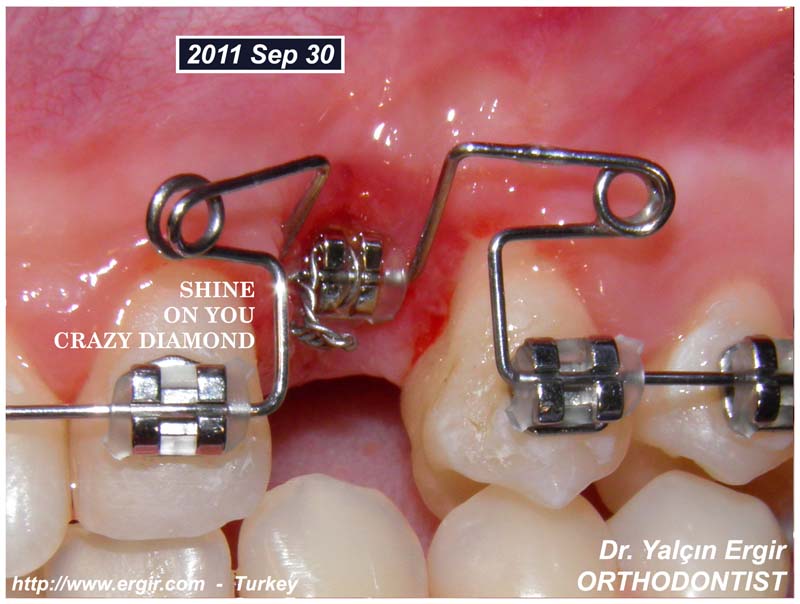
2011-09-30
biomechanic battle!...
This is a battle between bone tissue and orthodontic
forces. As no healthy bone structure with a healthy
periodontium can resist gentle and continuous
orthodontic forces - WE WILL WIN!
As the canine has erupted enough for the manually loop
bended stainless steel wires to be applied, we can begin
“Orthodontics’s Most Pleasant Application”= Bending
Loops
Loops cannot be formed in Titanium Wires, so we have to
use stainless steel wires for this oldie (but goldie)
edgewise technique.

When you take a close look at this shiny bends, the
deformation without irritating the gums can be seen and
the continuous force applied to the bracket can even be
felt in our heart.
When you make such a big deformation in applying the
wire to its bracket slot, I use:
one elastomeric chain circle - for one ear of the twin bracket
&
one
(Ø 0,25") stainless steel ligature wire -
for the other ear,
to ensure stability.
|
And it can clearly be seen
why we couldn't apply these loops before (2011 Aug 24)
as the bracket (our
diamond) was still
embedded in soft tissues:
|
wish you were here -
we will bring the diamond.
we are not only right
here waiting -
we are right here
fighting for you...
2011-10-26
3. month /
what as a speed & new horizons
What as speed this month - thanks to
"oldie but goodie" looped steel wires. Now it's time to
change the position of the bracket.

Before we could only bond a small
lower incisor bracket to the labio-distal part of the
canine because the labial surface was hidden behind the
palatinal surface of the lateral incisor tooth. With the
new position, we can bond it more medially and
gingivally, for more control, more force & less pandular
movement.
And back to Titanium wire again.
Today we have no pity; you can feel the great traction
force on the canine when you look at the deformation of
the wire. The the next 3-4 days will be a bit painful for
our dear patient - but it is worth it as it is safely and
gloriously coming - in "3 months", this view
is incredible.

From now on:
it is no more an "Impacted Tooth" for
us;
it is just (a bit severely) "Crowded
Teeth".
And no crowded teeth can resist to
Orthodontics -
we are winning - we are right here
waiting for you...
2011-11-17
4. month /
welcome party?
Can we get prepared for a "Welcome
Party"?
Hurraaaay! From now on we can even "brush"
the "no more-impacted" canine tooth -
even bite an apple at the 4th month
of the treatment.
Now the central-labial part is no
more under the bone and gingival tissues -
so we can debond the old bracket and
rebond it to the ideal position at the central part of
the labial surface.

With this new bonding, we take more
control
and can guide the canine to its
proper position and inclination in several months.
No elastic chain at this phase - the
teeth must be roughly aligned regardless of space or
crowding.
We will do the space "fine tuning"
afterwards.
 

Impacted tooth?
What impacted tooth??
We have just "Death Cab for Cutie"s
2005 single: "Crooked Teeth" at the moment
and we are right here listening...
2011-12-14
4 MONTHS + 3 WEEKS
2011/
July 22-August 24-September 30-October 26-November 17-December
14
WE ARE PROUD AS TURKISH ORTHODONTISTS
☺
Andrea Bocelli and Sarah Brightman is singing: Time To
Say Goodbye
and we are
singing:
Time to
apply rectangular NI-TI wire
(Ø .018" x .025")
Because we need torque control for a
tooth which has sailed a long distance,
 in the "Bone Sea of Palatina".
in the "Bone Sea of Palatina".

Alignment of teeth is not a two
dimensional operation. Teeth must be in harmonic
relation with the peripheral bony structures three
dimensionally.
While applying heavy torque forces to
the root, my advise is to firmly attach the rectangular
wire to the bracket slot by by tying a (Ø 0,25")
stainless steel ligature wire.

Without harming the periodontal
tissues and not devitalizing the tooth,
4 months + 3 weeks is a high-speed
biological period in erupting a fully impacted canine
tooth.
So; here is Hall's address,
if we want to take a "fast look" at
the
Dance of the Tooth-Plum Fairy:
http://www.ergir.com/2011/4_months_3_weeks.htm
2012-01-23
Now it is time for minor details in occlusion.

We are
all together at last; we can fly to the moon now - if
only we don't hurry taking the brackets
out. Fixed systems are always better than removable
systems but hygenically we have take to begin using
removable appliances - because fixed systems retain food
particules as well
(which may a cause tooth decay or severe periodontal
problems)
- as retaining a nice dental alignment.
The teeth have to fixed in their new positions and bone
structure for several "YEARS!”
inorder to prevent relapse problem.
****
THIS IS VERY IMPORTANT;
NOT FOR MONTHS -
BUT FOR SEVERAL YEARS!
You may ask: "why must a "completely impacted canine
tooth" be under retention for YEARS, if it can
orthodontically erupt in only 6 months’ time?
Relapse is a natural orthopedic response of the body
which cannot be overcame in several months.
So we must wait patiently and after 2 months we must
CONTINUE our treatment (retention) by invisible &
removable appliances,
INORDER TO BE -
HAPPY TOGETHER -
FOREVER....
** ** ** ** ** ** ** ** ** ** ** **
** ** ** ** ** ** ** ** ** ** ** ** ** ** ** ** ** ** **
** ** ** ** ** ** ** ** ** ** **
right here waiting…

dushekimi@ergir.com
** ** **
dr.
yalcin ergir - orthodontist
http://www.ergir.com |